So you have a meniscus tear. Now what?! Is surgery imminent, or can physical therapy help you?
Even though about 2 million meniscus procedures are performed worldwide each year, new evidence states that arthroscopic surgery is not more effective than physical therapy for some types of meniscal injuries.
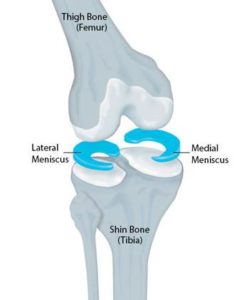
If you’re not sure what the meniscus is or what it does, check out this overview. Continue reading to find out:
- How a meniscus tear occurs
- How a meniscus tear is diagnosed
- Treatment of meniscus tears
- If surgery or PT may be indicated for a meniscus tear
How does a meniscus tear occur?
Meniscus injuries are fairly common and can be divided into either acute or degenerative categories.
Acute injuries usually happen in younger people and result from a combination of forces, such as loading and twisting the knee. Think of an athlete decelerating, then quickly changing direction to cut across a field.
Degenerative tears make up about 30% of all meniscus tears and are typically in older individuals. Accumulated stress to the knee over time makes the meniscus more susceptible to damage with small traumas, such as ‘taking a wrong step’ or twisting to get into the car.
How is a meniscus tear diagnosed?
There are a few quick, hands-on tests that can be done to make healthcare clinicians suspect injury to this structure. No single clinical test can make the diagnosis, but a cluster of tests can predict it. A group of tests established in 2006 included the following:
- History of joint locking (the knee may feel stuck in one position)
- Joint line tenderness (painful when pushing in certain areas around the knee)
- Positive McMurray’s test (maneuver where the clinician bends and then straightens your knee while pushing inward or outward)
- Pain with flexion overpressure (pushing on a bent knee)
- Pain with extension overpressure (pushing the knee into a straight position)
If most or all of these cause you pain, the likelihood of a meniscal tear increases, but you’d still need imaging to confirm the diagnosis.
As far as types of imaging procedures, X-rays generally aren’t helpful – you don’t really see the meniscus on standard x-ray pictures. The most accurate way to diagnose meniscal injury is with MRI. Ultrasound or CT may also be used, but are less common since MRI is pretty darn good at identification of these injuries.
Fun fact about meniscal injuries: Tears are actually frequently found on imaging in people WITHOUT symptoms (it’s estimated that 36% of people without any knee pain have a tear!). So it is possible to have one found on imaging, without having pain. Some meniscus tears may just be a normal part of structural changes that go along with aging.
How are meniscus tears treated?
A few options for treatment exist, including conservative rehabilitation and a few different types of surgery. The decision is based on your age and the type of tear. Often, conser and include pain control, modifying your activities, and range of motion exercises before progressing to strength and functional activities.
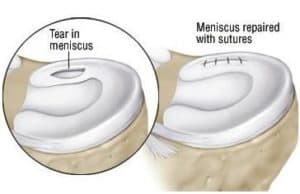
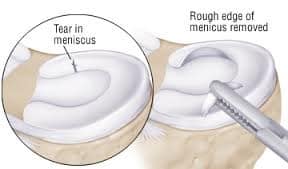
You may need surgery if you have a very large tear, or one that causes the knee to lock. Surgery could involve one of the following: repair, removal, or in rare cases, replacement.
Your meniscus would likely be repaired if the tear was located on the outside region of the meniscus. There’s better blood-flow here, meaning a greater capacity for healing.
Meniscus removal (also known as meniscectomy) is usually indicated if you have a tear in the middle of the meniscus. Very little to no blood-flow in this region means it’s less likely to heal. Usually and when possible, a partial meniscectomy is performed – meaning just part of the tissue would be removed, not the entire thing. Meniscectomy has a faster post-operative recovery time than meniscus repair, but greatly increases your risk for arthritis down the road.
Meniscus replacement, though uncommon, may be an option for young, active people who previously had the meniscus removed.
Do I need surgery or PT for a meniscus injury?
Current evidence states that the first treatment for degenerative meniscus tears should be physical therapy! Several studies have shown that improvements in pain and function are the same whether you have arthroscopic surgery or physical therapy. Long-term, those with a history of arthroscopic meniscectomy are 3 times more likely to get a knee replacement later in life – meaning that it’s in your best interest if surgery can be avoided!
Based on these results, physical therapy sounds like a pretty fantastic alternative to surgery if you have a degenerative meniscus tear that’s causing you pain.
Keep in mind there are absolutely still instances when surgery is necessary and has great outcomes. This is a decision that will be made by you and your physician based on the type of tear and your age. When surgery is needed, post-operative physical therapy is often recommended to get you back to your favorite activities safely and effectively.
In summary, you’re not doomed to surgery or a future knee replacement if you have a meniscus tear – physical therapy is able to reduce pain and improve function, and is highly recommended as a first line of treatment. If you’d like more guidance on your knee pain, we’d love to help out! Give us a call today, and get started on your own rehab journey with our tips for managing knee pain.

References
Logerstedt, D. S., Snyder-Mackler, L., Ritter, R. C., Axe, M. J., Godges, J., Altman, R. D., … & Fearon, H. (2010). Knee pain and mobility impairments: meniscal and articular cartilage lesions: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy, 40(6), A1-597.
Lowery, D. J., Farley, T. D., Wing, D. W., Sterett, W. I., & Steadman, J. R. (2006). A clinical composite score accurately detects meniscal pathology. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 22(11), 1174-1179.
van de Graaf, V. A., Noorduyn, J. C., Willigenburg, N. W., Butter, I. K., de Gast, A., Mol, B. W., … & Poolman, R. W. (2018). Effect of early surgery vs physical therapy on knee function among patients with nonobstructive meniscal tears: the ESCAPE randomized clinical trial. JAMA, 320(13), 1328-1337.
Zanetti, M., Pfirrmann, C. W., Schmid, M. R., Romero, J., Seifert, B., & Hodler, J. (2003). Patients with suspected meniscal tears: prevalence of abnormalities seen on MRI of 100 symptomatic and 100 contralateral asymptomatic knees. American Journal of Roentgenology, 181(3), 635-641.









































")

")








{kind=link}